The Code Room Has a Medication Safety Problem No One Has Solved. Until Now.

Early in my career, I gave a young girl ten times the dose of epinephrine she needed. The error was mine. She survived, but I have never forgotten what it felt like to be the one who made it, or how easily it happened.
Over the past two decades, I have run codes in emergency departments. I have stood at the head of the bed and called out drug orders in a room that is loud, fast, and unforgiving. I have watched nurses draw up medications from memory, from habit, and from whatever vial was closest. I have seen the right drug pulled in the wrong concentration. I have seen verbal orders misheard. I have seen the system work, and I have seen it fail quietly, with no alarm, no alert, and no record.
We talk a lot about medication safety in hospitals. We have built extraordinary infrastructure around it. Pharmacy verification. Automated dispensing cabinets. Electronic medication administration records. Barcode scanning at the bedside.
And yet there is one room where almost none of that applies.
The code room.

After two decades, I think we finally have an answer. But to understand why it took this long, you have to understand why the problem was so hard to name.
What barcode scanning actually requires
Modern hospital barcode scanning is built on a specific chain: a physician enters an order in the EHR, pharmacy reviews and verifies it, a pharmacist-prepared product with a hospital-generated label arrives at the bedside, and the nurse scans that label against the active order to confirm the right drug is going to the right patient.
It is a good system. When it works, it works well.
But in a resuscitation, that chain does not exist.
There is no order in the EHR - not yet, sometimes not ever. There is no pharmacy in the loop. There is no pharmacist-prepared bag. The nurse is drawing up epinephrine, amiodarone, or norepinephrine from raw vials, in real time, under enormous pressure, based on a verbal order called across a crowded room.
In that moment, the barcode scanning infrastructure that the hospital spent millions of dollars building is completely irrelevant. There is nothing to scan against. There is no verified order to close the loop on. The safety net has a hole exactly where the patient is most vulnerable.
The RaDonda Vaught case is a symptom, not an anomaly
In 2017, nurse RaDonda Vaught administered vecuronium instead of Versed to a patient at Vanderbilt University Medical Center. The patient died. Vaught was ultimately convicted of criminally negligent homicide.

The case drew fierce debate in the nursing community, and rightly so. Many argued, correctly, that the conditions that led to her error were systemic: an overridden cabinet alert, a broken safety culture, a high-stress environment, and a series of small failures that compounded into a catastrophic one.
What rarely gets named directly is this: in high-acuity, time-compressed clinical moments, human beings make errors. Not because they are careless. Not because they are undertrained. Because the environment exceeds what human cognition can reliably handle alone.
Vaught’s case happened in a hospital. With infrastructure. With systems. And still, a wrong drug reached the patient.
Now ask yourself what happens in a room with less infrastructure, more chaos, and no scanning at all.
The gap no one is solving, and why it has been so hard
I have spent years in emergency medicine and even longer thinking about medication safety in high-acuity environments. And the gap I keep coming back to is not in the pharmacy. It is not in the dispensing cabinet. It is at the bedside, in real time, when the drug is in someone’s hand and no system in the world is checking it.

The reason this gap has persisted is not lack of awareness. It is a technical problem that most people have not fully named.
Barcode scanning in hospitals works because it has something to scan against - a physician order, a pharmacist-verified product, an active entry in the EHR. The scan is a confirmation step at the end of a verified chain. Remove the chain, and the scan has nothing to do. It becomes a camera pointed at a vial with no reference point, no context, and no way to know if what is in that vial is the right drug at the right concentration for this patient right now.

That is why the code room has been unsolvable. Until you have a reference point that does not depend on an EHR order, you cannot do barcode verification in real time resuscitation.
The Breakthrough
The solution, it turns out, was not a scanning problem. It was a data problem.
More than a decade ago I had a single clinical insight that remains at the core of everything we build: every drug used in the code room must be predetermined. Every dose, for every weight, for every patient - push medications, infusions, and equipment - selected, calculated, and clinically verified in advance with the hospital’s clinical and pharmacy team. That is not a small thing.
And it turns out that predetermined data layer is exactly what barcode scanning needs to work without an EHR order. When a clinician opens the app during a code, there is nothing left to compute. That is the entire reason orderless barcode verification is possible, and why no one has been able to do it before.
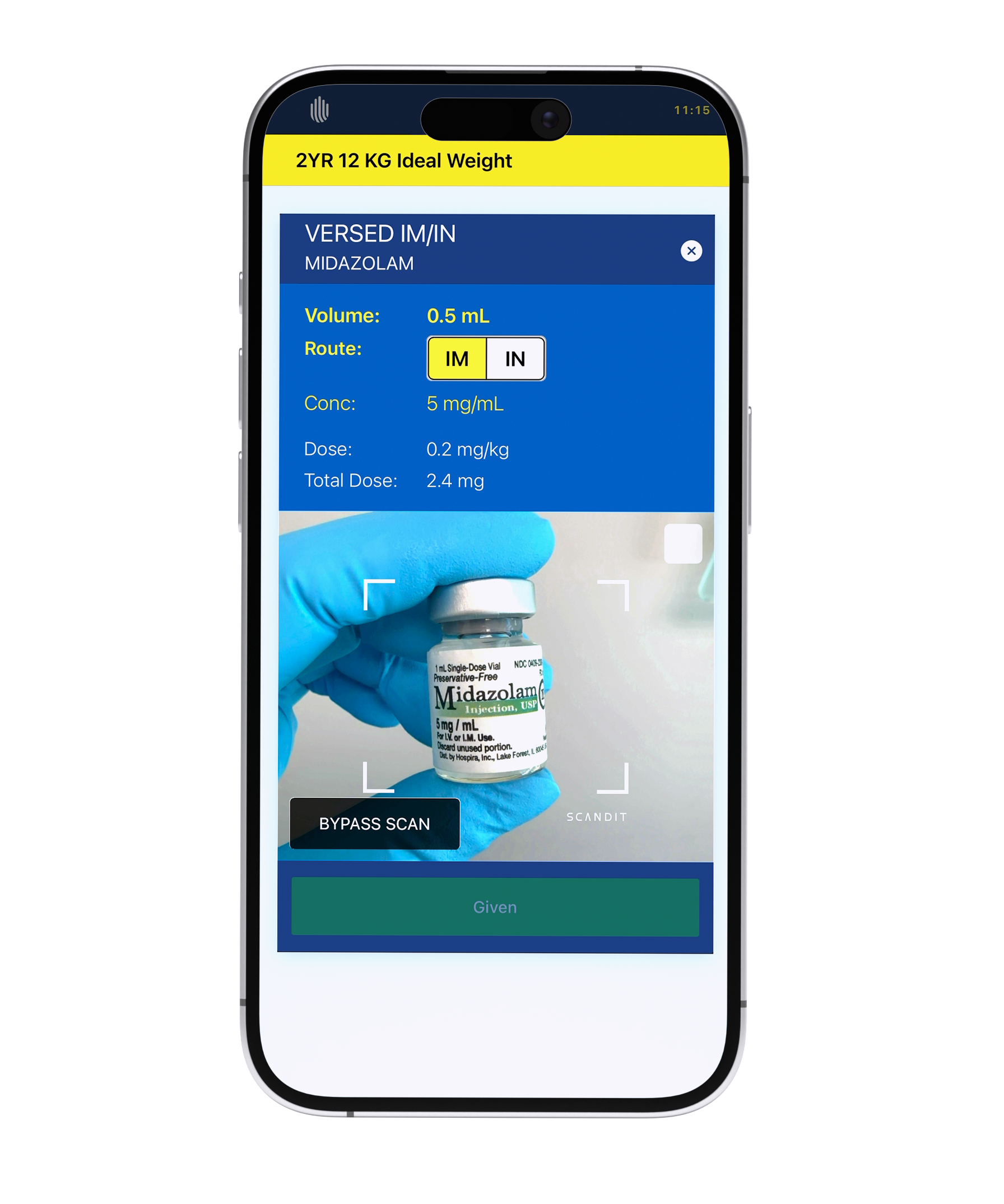
When a clinician selects a medication in our system, the correct drug and the correct concentration are already known. That becomes the reference point. When they scan the vial, the system checks what is in their hand against what should be in their hand - in real time, at the bedside, with no pharmacy loop and no physician order required.
This is ScanSafeTM. And it is, to my knowledge, the first-time barcode medication verification has been made available in an orderless environment.
The predetermined data architecture that we built to eliminate dosing errors also eliminated the dependency that made scanning impossible in resuscitation. Those two things, dose calculation and barcode verification, turn out to be the same problem, solved together.
For EMS clinicians who have never had any of this infrastructure, it is a meaningful leap forward. For nurses and emergency physicians running codes, it closes a gap that hospital scanning systems were never designed to address.
The room that needs barcode scanning the most finally has it.
How many errors will happen now that RQI exists...and it exists outside the hospitals as unattended kiosks 24 hour access for BLS ACLS PALS and its a 2 year card off the same RQI system. No team interaction and I can have all 3 cards in about 15 minutes.